This is a two-part series on Parkinson’s, detailing the daily struggles with the disease, new treatment programs and how patients’ lives have been impacted by emerging therapies. You can read the first part here.
The night before he had brain surgery to treat his Parkinson’s disease symptoms, Robert Goings couldn’t sleep.
“He was pacing all night,” says his wife, Diana. That’s because it hurt to stop moving. Normally, Goings’ restless movements, stiffness and muscle cramps were eased by medicine. But doctors wanted his symptoms unmasked for the procedure, which meant he was feeling them full blast. “My legs would cramp up, my arms, you know, everything would cramp up without the medication,” Goings says.
The next morning, last November 5, Goings, who at age 68 had been living with increasingly disruptive symptoms for years, slid into an MRI machine at Oregon Health and Science University, or OHSU, in Portland. While Goings was inside the MRI tube, doctors aimed 1,024 ultrasound beams at several spots deep in his brain, burning the problematic tissue there.
Afterward, Goings was wheeled to a recovery room. “He held out his hand — dead still,” Diana says. She remembers thinking, “Oh my God, I don’t believe this. It’s gone. Absolutely gone.”
In opting for this treatment, called high-intensity focused ultrasound, Goings has joined a small but growing number of people choosing to control their Parkinson’s symptoms with permanent lesions in their brain. Already, an estimated 50 to 60 people have undergone the surgery at OHSU, where the treatment calendar is booked up months in advance.
The U.S. Food and Drug Administration approved the earliest version of the treatment for certain Parkinson’s patients in 2018, with several key clinical trials showing positive results. The latest version, which Goings received, was approved in 2025 and extends the treatment to include a new target in the brain that seems to ease not just tremors but also other movement symptoms, including slowness and stiffness. What’s more, the treatment can now be done to both sides of the brain, thus providing relief to the entire body.
“People go into it not believing,” says neurosurgeon Daniel Cleary, who has been helping to lead the focused ultrasound efforts at OHSU and who performed Goings’ procedure. But the before-and-after experience can be profound.
Data generated in a yet-to-be published clinical trial of 40 people show that, when delivered to both sides of the brain, the treatment can improve people’s movement disability symptoms by an average of about a third. That’s compared with symptoms when patients are not taking medication. Three months out, 86 percent of study participants felt that overall, their Parkinson’s symptoms had improved.
Many of the patients Cleary treats have had tremors for years, even decades. When they come out of the procedure and look at their hand, they are amazed that it’s not shaking anymore. “Families get very emotional,” Cleary says. “The patients get emotional. We get emotional. It’s a big thing.”
High-intensity focused ultrasound for Parkinson’s is not yet widely available. In the United States, mainly large academic centers have the expertise to do it, Cleary says. And because the technique is relatively new, questions remain about the long-term effects. Like other Parkinson’s treatments, the method relieves symptoms but it doesn’t stop or even slow the brain destruction caused by the neurodegenerative disease.
Still, the procedure, which involves no cutting into the head, no anesthesia and no recovery in a hospital, holds promise as a way to ease severe symptoms for millions of people with Parkinson’s worldwide.
On their way north to OHSU from their house in Lebanon, Ore., Robert and Diana drove through a violent rainstorm, with poor visibility and lots of curves. Robert was driving, though they had taken Diana’s car, expecting her to drive home. On the day after his procedure, Robert was feeling so good that he drove them both home.
Neuroscience at work
Parkinson’s is marked by the death of a cluster of nerve cells deep in a part of the brain called the substantia nigra. These cells make the chemical signal dopamine, a neurotransmitter that’s crucial for movement. One of the most common treatments is a medicine called levodopa, which adds back some of the missing dopamine. Other medications include carbidopa, which boosts levodopa’s effects, and other drugs that influence the brain’s dopamine system. While these medicines can help tremendously, Parkinson’s is relentless. As the disease progresses, the drugs become less effective and increased dosages can cause debilitating side effects like uncontrolled movements.
Once Parkinson’s progresses to later stages, some people opt for a treatment called deep brain stimulation, or DBS. Like a pacemaker for the brain, an implanted DBS system stimulates nerve cells in a way that can reduce symptoms. But some people aren’t eligible for the surgery because they’re not healthy enough, or they don’t want permanent implants that require ongoing medical management.
Focused ultrasound gets around some of those issues by using a helmet that can dispense 1,024 ultrasound beams. The sound waves — the same sort that produce babies’ sonograms — enter the head, pass through the skull and intersect at a precise spot deep in the brain. During the procedure, which lasts a little under an hour, doctors use the heat those waves create when they intersect to make a lesion.
“Ultrasounds are just mechanical waves — the same thing as if you drop a stone in a pond,” says Pablo Villoslada, a clinical neurologist at Hospital del Mar in Barcelona who is exploring less intense ultrasound waves to treat dementia, multiple sclerosis and amyotrophic lateral sclerosis, or ALS. Because the waves can, in principle, reach anywhere in the brain, ultrasound methods hold promise for all sorts of neurological and mental health ailments, such as eating disorders, mood disorders and chronic pain, he says. “You need to select the right target, the right patient, the right circuit, the right stimulation,” he says. “A lot of research must be done, but the potential is very high.”
As a young man in his early career, Goings trained as a Navy diver, going deep underwater in Pearl Harbor, the bottom of which was a perpetual mud pit churned up by big ships. Some training exercises were done in the dark. He wore a blacked-out Mark V diving helmet, rendering him totally sightless. “You have to be able to feel,” Goings says. Steady hands. No panicking.
For his procedure, Goings was in a different sort of helmet, though water was still involved. Before getting started, medical staff shaved his head and mounted it in a tight-fitting brace. Screws that poked into his skin held everything steady. The procedure was done in an MRI so that Cleary and his colleagues could find the right spots to hit. And before Goings went into the machine, a flexible bladder sitting on the top of his head was pumped full of water. The liquid had two jobs: It helped conduct the sound waves into the head, and it helped keep his head from heating up under the beams. Throughout the procedure, clinicians slid Goings in and out of the MRI tube several times to test his symptoms.
There’s a lot of intricate neuroscience behind the focused ultrasound technique, says Delaram Safarpour, a neurologist and movement disorder specialist at OHSU. Movement results from a complex web of neural areas that span the brain. Some of these areas hit the gas pedal for movement, and some throw on the brakes.
“It’s a big circuit that has to work in a balance,” Safarpour says.
In Parkinson’s, too much braking in one circuit can interfere with other parts of the network. “People will start having more movements than they should,” Safarpour says. Taking out one of the brakes with ultrasound “is cutting a part of the circuit in order to bring the balance back.”
Two such braking regions are ultrasound targets. The first, called the ventral intermediate nucleus of the thalamus, or VIM, is a good target for people who get tremors when they try to move. That issue can be present in Parkinson’s, and it is a key symptom of a condition called essential tremor. The brain circuit that controls tremors involves signals moving from the cerebellum at the back base of the brain all the way up front to the motor cortex.
“We don’t fully understand how the brain circuits work that affect tremor,” Cleary says, but “we know that if we can knock out part of that pathway, the tremors get better.”
A second target, the pallidothalamic tract, or PTT, is central to the latest FDA approval. A lesion there can ease slowness, stiffness and involuntary irregular movements called dyskinesia. It can also ease the pain caused by constant tensed-up, taut muscles that is almost universal among Parkinson’s patients. “Because they’re so rigid, so locked in, they get really severe pain,” Cleary says.
Goings’ tremors were worse on his right side, which is controlled by the left side of his brain, so that’s where doctors aimed. Cleary generally targets both the VIM and the PTT. The procedure is done in stages, first with the ultrasound intensity high enough to temporarily disable the tissue but not permanently burn it. That lets doctors test the spot to see if the patient experiences relief before creating the permanent lesion.

“There was one point about three quarters of the way through, I came out of there smiling,” Goings says. He was grinning because he felt his symptoms improve. “I said, you got the right spot,” he says.
Diana remembers the doctor replying, “Oh no, we can do better than that.” They did.
Goings’ symptoms on the right side of his body have eased dramatically since his procedure, he says. “There are no ands, ifs or buts about it,” he adds. “I am one hundred percent no regrets.”
As with many other patients who get the procedure, Goings has remained on his medications, with the ultrasound treatment offering an added benefit. He’s waiting now to have the other side done, which requires at least a six-month wait while doctors see how he’s responding to the first procedure.
Still early days
Others have reported similar success. During his procedure, Gary Gilson, a 68-year-old former surgical assistant who lives in Hillsboro, Ore., was shaking so hard that technicians used weights and straps to keep him still. The shaking was expected, since he hadn’t eaten much and hadn’t had any medication. But what happened next surprised him. “All of a sudden, it just stopped … I was fighting it and then the next thing you know, it was gone.”
Career changes

Both Robert Goings and Gary Gilson say their Parkinson’s played a role in their retirement. Gilson, a former surgical assistant, eventually retired earlier than planned. Goings, who had worked as a draftsman and then a civil engineering technician, experienced changes in his lettering and was often tired and ill from his medication. “The symptoms kept getting worse, and I actually retired at 62,” Goings says. “A portion of the decision in retiring was the Parkinson’s.”
In the three months since, Gilson’s tremors have improved, but the biggest difference is that the pain that used to come from muscle rigidity on his right side has largely disappeared, he says. Because his left side wasn’t as symptomatic as his right, he and his doctors are waiting to decide whether he will go back for treatment on the other side.
Linda Grant, from the small mountain town of Sisters in central Oregon, was similarly worn out from tremors. “My body fights every single tremor I have. My brain wants to stop it. So I think that’s what tires me out so much. It’s exhausting, actually.”
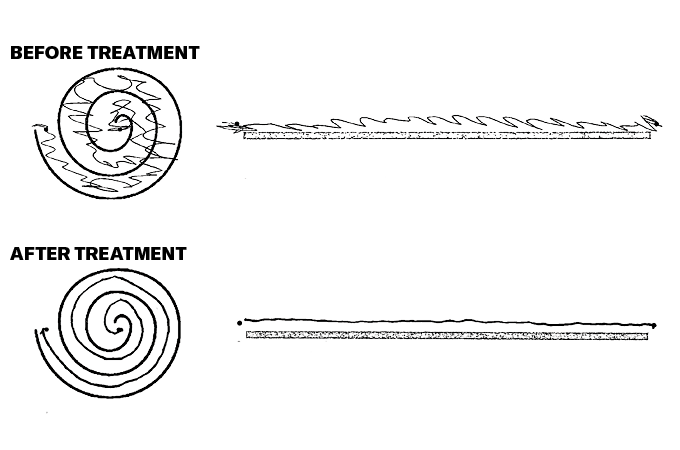
Each time Grant came out of the MRI tube during her procedure, the clinicians would test her symptoms by asking her to use a stylus pen to trace a spiral and draw lines on a tablet. Throughout her procedure, her lines got more precise, steadier. Her tremors eased. Her right arm grew less rigid.
Afterward, as she settled into a recovery room, a nurse handed Grant a cup with no straw. Before her procedure, she wouldn’t have been able to drink from it easily. But now she could. In the months since her treatment, Grant’s tremors in her right hand have improved, though she still experiences tremors there when her left side shakes.
A common side effect of the procedure is temporary balance problems, lasting a few weeks to months, Cleary says. But those typically clear up and leave a person sturdier, he says. Grant has experienced some trouble walking, and has been working hard in physical therapy to keep herself as strong and mobile as possible. As for whether she’ll have the other side treated, she doesn’t hesitate: “I can’t wait.”
Nurse manager Christine Larsen, a coordinator of the focused ultrasound program at OHSU, checks in with patients after their procedure. She usually asks how their night went. She remembers one man answering that he had slept without waking for the first time in 20 years.
His wife said, “I woke up and I thought he was dead, because I’m used to sleeping with somebody who’s in constant movement, constant tremor.”
Data from patients treated for essential tremor, reported in 2022 in the Journal of Neurosurgery, show that improvements can last for at least five years — which is as long as patients have been followed so far. But how long relief might last for Parkinson’s patients is not at all clear.
Parkinson’s does not stop. Along with the death of nerve cells in the substantia nigra, other changes unfold over time. A sticky protein called alpha-synuclein clumps up, and that clumping spreads elsewhere in the brain, interfering with brain activity. Systems that handle smell and digestion become disordered.
It’s against this relentless body-wide backdrop that people are searching for relief, for as long as they can get it. While brain lesions created by focused ultrasound are not a cure for Parkinson’s, the approach can help people get through their days. “It’s a tough disease,” Cleary says. “This makes a huge difference in their life.”
These are early days, and there are a lot of questions to answer. Efforts include learning more about which patients might benefit the most, when to treat them and how to choose targets in the brain for each person. Plans are in the works to further study the PTT as a Parkinson’s target. All the while, scientists are searching for ways to stop or slow the disease itself.
Cleary and other doctors at OHSU have busy schedules. They perform the procedures every Wednesday and every other Monday, usually treating about five people a day.
Cleary sees access as one of the biggest hurdles: Many people don’t know that focused ultrasound is an option, there aren’t enough surgeons and clinicians trained to do the procedure and the cost is not always covered by health insurance.
Making a compelling case to insurance companies requires more data, Safarpour says. “In big centers like ours, we constantly are gathering important data from patients that go through these procedures, and these will all become scientific papers that show improvement in quality of life and symptoms,” she says. When it comes to insurers, “that’s the way to fight back.”
Though there’s more work to do, the future for people with Parkinson’s seems brighter than it did a decade ago, Cleary says. The first patient he treated with the new approach went from being unable to walk well to fluidly walking down the hall. “Seeing the profound effect on this single patient has really inspired a lot of people to say, ‘OK, maybe we should go forward with this. Maybe this is something that’s really powerful,’ ” he says.
When I ask Gilson, the former surgery technician, what’s next for him, he answers immediately: “I’m going on vacation with my wife.” They plan on visiting England, Germany and the Netherlands. The Gilsons have also bought a camper for future trips.
Goings is keeping busy closer to home, with firewood that needs chopping and rambling walks with his dog Scooter. Diana says that when faced with a challenge, Robert is the guy to say, “Give me some more.” In this way, his Parkinson’s is no different than any other challenge.
“There’s no cure for it right now,” Goings says. “But this is as close as I think you’re going to get.”